
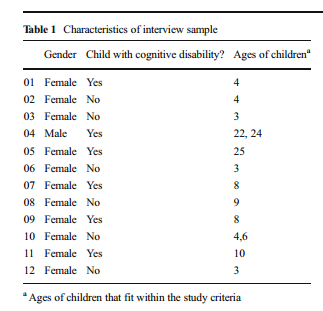
Participants were 12 parents – 6 with children who had intellectual disability (CD) – 6 who did not (ND) and whose children were between the ages of 3-9
6 THEMES EMERGED FROM THE INTERVIEWS:
MEANINGS OF HEALTH AND TREATMENT
ROLE OF MEDICINE
HARM
THE “GOOD” PARENT
NORMALITY & SELF-PERCEPTION
Some of the parents were attracted to CE products in order to their child feel more normal, because the real or perceived abnormality was harming their child emotionally or socially. However, parents found it hard to strike a balance between achieving normality while still encouraging their child to accept themselves for who they were. Both groups of participants expressed worry that encouraging their child to take CE products would leave their child feeling ‘broken’ or incomplete as a person, even when the intention of the products was to mitigate their child’s suffering.
ABILITY
DISCUSSION / CONCLUSIONS
“Parents viewed themselves as being responsible for avoiding harm in their child’s life wherever possible and risking harm for their child for the purposes of CE was seen as unacceptable to all participants in this study.”
Compared to other studies, parents in this one were more concerned with changes in identity of the child that came from a perceived message they would be sending by encouraging or forcing their children to use CE products in order to be “loved, happy, successful and complete.”
There were more similarities than differences between the parent groups. One important difference was that parents of children with a CD were able to give concrete examples, not hypothetical stories, of what it is like to see your child struggle and firsthand experience with pharmaceutical interventions. They also: “expressed that the way society was structured often worked against their child because of their ability differences, and as a result, sometimes they felt desperate and used approaches that they may not have even considered previously.”
For purposes of this study, CE was defined as interventions that would create “above average” results. Parents on the other hand continuously referred to the interventions as being disability based and used to mitigate struggle. Using CE products for children who did not have a disability or disease was unacceptable because they could: “damage a child’s self-esteem, run the risk of putting the child’s physical health in jeopardy, and/or perpetuate unhealthy levels of cognitive competition between children.”
Products not marketed as being medical treatments would be more popular.
Results suggest that parents who push their children to use these products will be stigmatized by other parents who view them as “being too preoccupied with outward appearance, overly competitive, and failing to care properly for their child.” This is multiplied for the use of CE when children have less autonomy (as the case with children who have a disability) and brings up the issue of CE products being used in secrecy.
Parents in this study suggested that they would rely on physicians to know the risks and benefits of these products and be able to monitor their use. Physicians have reported in the past that they may not feel comfortable with prescribing these products because of the lack of available information – scope of their practice.
Terms such as ethics, or ethical treatment were not used once by participants in this study. The only reference made to moral decisions was made in reference to not judging parents who use the products.
Researchers talked about the future of CE products and more wide-spread use. Implications including the idea that use by “typical” children to obtain above average intelligence may negatively affect people with CD, creating further stigmatization and competition for services.